
by Robert Yeakel / NGA, director of government relations
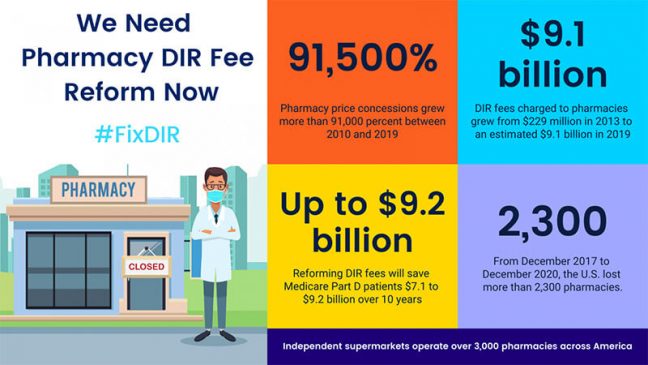
Independent supermarkets operate more than 3,000 pharmacies across the country. In many small towns and rural areas, the grocery store pharmacy is the only healthcare provider in the community.
In recent years, two disturbing trends have been accelerating: Medicare Part D beneficiaries are paying higher out-of-pocket costs, and independent community pharmacies are closing. This is a direct result of pharmacies being assessed ever-increasing direct and indirect remuneration (DIR) fees. These fees, often referred to as “rebates” or “price concessions,” are abused by Part D plan sponsors and pharmacy benefit managers to strategically recoup funds from pharmacies long after transactions have been completed.
DIR fees are unpredictable and seemingly unconnected to a pharmacy’s performance or other standards. According to recent Centers for Medicare & Medicaid Services data, DIR fees grew by more than 91,500 percent between 2010 and 2019. Independent supermarket pharmacies have virtually no ability to absorb or budget for these unexpected costs.
Even worse, because DIR fees are regularly applied to the price of a drug long after the point of sale, patients do not benefit and end up paying a larger share of the actual cost of the drug.
Pharmacy DIR reforms have enjoyed bipartisan support in both the House and Senate. In the 116th Congress, important Part D DIR fee reforms were included in House-passed and Senate Finance Committee-passed drug pricing legislation.
Just a few weeks ago, a bipartisan coalition of both House and Senate pharmacy champions introduced updated legislation. The Pharmacy DIR Reform to Reduce Senior Drug Costs Act (H.R. 3554 / S. 1909) seeks to lower cost sharing for Medicare Part D patients and ensure that community pharmacies continue to provide vital healthcare access to millions of Americans.
NGA and our pharmacy coalition partners are reaching out to members of Congress and asking them to cosponsor the legislation.
Additional Info and How to Take Action
To take action and for additional resources, click on the following links:
To view a current list of cosponsors: R.3554 / S.1909
Ask your members of Congress to cosponsor the bill: NGA’s Grocers Take Action Center.
To send a company letter directly to your members of Congress, download: Sample House Letter / Sample Senate Letter
Click here to view and download an issue brief on the bill.
Click here to view a section-by-section of the bill
Save the graphic below and use on your social media with the hashtags: #FixDIR and #DIRisDIRE
Data Points Supporting DIR Fee Reform
From December 2017 to December 2020, the United States lost more than 2,300 pharmacies, according to data from IQVIA.
A 2020 Drug Channels report found that DIR fees charged to pharmacies grew from $229 million in 2013 to an estimated $9.1 billion in 2019.
“Pharmacy price concessions account for a larger share than ever before of reported DIR and thus a larger share of total gross drug costs in the Part D program. The data show that pharmacy price concessions, net of all pharmacy incentive payments, grew more than 91,500 percent between 2010 and 2019.” – Centers for Medicare & Medicaid Services, Fiscal Year 2022: Justification of Estimates for Appropriations Committees (published June 2021).
“When pharmacy price concessions are not reflected in the price of a drug at the point of sale, [patients] do not benefit through a reduction in the amount they must pay in cost-sharing, and thus end up paying a larger share of the actual cost of a drug.” 83 Fed. Reg. 231, 62174 (published Nov. 30, 2018).
DIR reform reduces patient cost sharing for medications. Reforming pharmacy DIR fees will save patients $7.1 to $9.2 billion over 10 years. 83 Fed. Reg. 231, 62154 (published Nov. 30, 2018)
DIR reform increases medication adherence. A review of 160 studies revealed that medication adherence significantly decreases as medication costs to the patient increases. Eaddy MT, et al. “How patient cost-sharing trends affect adherence and outcomes.” Pharmacy & Therapeutics, January 2012.
DIR reform allows patients to stay healthier and avoid more costly care. Disease-specific cost of non-adherence is estimated up to $44,190 per person, and costs attributed to “all causes” non-adherence is estimated up to $52,341 per person. Cutler RL, et al. “Economic impact of medication non-adherence by disease groups: a systematic review.” BMJ Open, January 2018.
DIR reform lowers overall healthcare costs, saving the federal government money. If the 25 percent of non-adherent hypertension patients became adherent, Medicare could save nearly $14 billion annually, averting more than 100,000 emergency room visits and 7 million inpatient hospital days. Lloyd JT, et al. “How much does medication nonadherence cost the Medicare Fee-for-Service Program?” Medical Care, 1/2019.
If you have any questions, or for more information, contact Robert Yeakel at [email protected].